
{kind=link}
Your shin begins burning at precisely the identical level in each run.
Mile two, typically mile three.
The ache is deep contained in the muscle, not on the bone.
It fades fully inside 20 minutes of stopping.
That sample is the hallmark of persistent exertional compartment syndrome, a situation that seems to be like shin splints from the skin however works in a different way beneath.
Prognosis takes months on common as a result of the ache vanishes by the point you attain the physician’s workplace, and most clinicians don’t measure compartment stress until prompted.
On this article, you’ll study:
- How compartment syndrome differs from shin splints primarily based on location, timing, and bilateral patterns
- What triggers the stress buildup in runners and who faces the best danger
- How docs verify the prognosis utilizing a stress check after train
- Whether or not surgical procedure is critical, and what a 2012 research suggests a few non-surgical different
- How shortly you’ll be able to return to working after remedy
Is It Compartment Syndrome or Shin Splints?
Each accidents produce lower-leg ache that worsens with working and each are widespread in distance runners.
The vital distinction is anatomical: shin splints (medial tibial stress syndrome) trigger ache instantly on the shin bone, whereas compartment syndrome causes ache contained in the muscle stomach a number of centimeters away from the tibia.
In case your ache sits instantly on the ridge of the shin bone relatively than deep within the muscle tissue a number of centimeters away from the bone, shin splints or a stress fracture is extra seemingly than compartment syndrome.
Timing is the second differentiator.
Shin splints usually damage from step one, and soreness can persist for hours after a run.
Compartment syndrome has a dependable onset window: you’re pain-free for the primary mile or two, ache builds steadily till you cease, after which it clears inside half-hour of ending.
A 3rd clue: compartment syndrome impacts each legs concurrently in 60 to 80 p.c of circumstances.
Bilateral muscle ache that seems on the similar distance every run, deep within the muscle, with speedy post-run decision is the traditional compartment syndrome profile.
What Causes Compartment Syndrome in Runners?
The muscle tissues of your decrease leg sit inside 4 tight sheaths of connective tissue known as fascial compartments.
Once you run, blood circulation to working muscle tissues will increase and so they swell by as a lot as 20 p.c in quantity.
In most runners, the compartment is massive sufficient to accommodate this growth with out difficulty.
In runners with persistent exertional compartment syndrome, the fascial sheath is just too inflexible relative to muscle quantity.
Strain contained in the compartment rises sharply throughout train, compressing blood vessels and nerves and producing ache that forces you to gradual or cease.
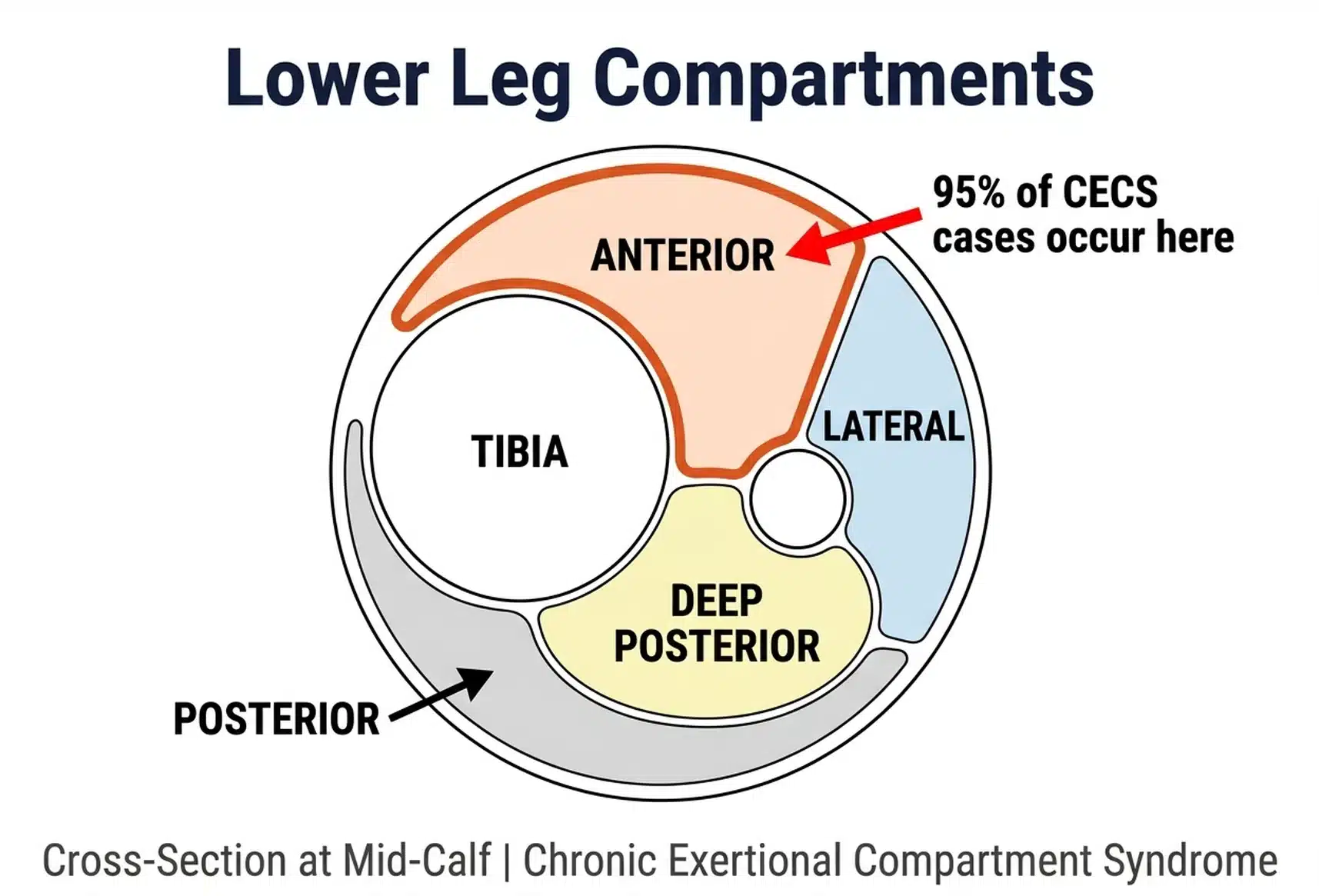
Analysis has discovered that 95 p.c of persistent exertional compartment syndrome circumstances happen within the anterior or lateral compartments of the decrease leg — the entrance and outer shin.
This focus within the anterior compartment issues for remedy: the surgical strategy and even the non-surgical choices differ primarily based on which compartment is affected.
Compartment syndrome is extra widespread in youthful runners.
The median age at symptom onset is round 20 years, which is sensible anatomically: the scale of your fascial compartments is mounted as soon as development stops, and issues are inclined to emerge when coaching quantity climbs post-adolescence.
Women and men develop it at roughly equal charges.
Some proof hyperlinks rearfoot putting and overstriding to increased loading of the anterior compartment, although that is primarily based on biomechanical information relatively than potential harm monitoring.
What Are the Signs of Compartment Syndrome?
The situation of your signs will depend on which compartment is concerned.
Anterior compartment syndrome produces aching, tightness, and burning throughout the entrance and barely outer face of the decrease leg, the fleshy space simply to the skin of the shin bone.
Posterior compartment syndrome, which is rarer, produces comparable signs within the calf and again of the decrease leg.
Throughout every kind, the hallmark options are:
- Ache that begins after a predictable distance or length, usually the identical level each run
- Progressive worsening that forces you to gradual or cease
- Full or near-complete decision inside 15 to half-hour of stopping
- Tightness, numbness, or tingling within the foot or decrease leg throughout train
- Weak spot when attempting to tug your toes upward (anterior) or push by way of a calf increase (posterior)
Ache that disappears inside minutes of stopping and returns on the similar level in each run is probably the most dependable single symptom of compartment syndrome, and the function that almost all clearly separates it from shin splints or a tibial stress fracture.
In some circumstances, you’ll really feel agency, swollen lumps alongside the muscle stomach throughout or instantly after a run because the muscle presses towards the restricted fascia.
How Do Docs Diagnose Compartment Syndrome?
Diagnosing compartment syndrome in a clinic is notoriously tough as a result of the ache disappears shortly as soon as train stops.
An MRI or bone scan can rule out tibial stress syndrome and stress fractures, each of which present up clearly on imaging, however neither confirms compartment syndrome.
The gold-standard check is a compartment stress measurement carried out instantly after train.
The protocol: you run on a treadmill till you reproduce your signs, then a doctor inserts a needle-tipped stress gauge into the affected compartment and data readings inside one to 5 minutes of stopping.
Strain above established thresholds on the one- and five-minute marks confirms the prognosis.
Appropriate prognosis takes a number of months on common as a result of ache resolves earlier than most appointments. When you have traditional compartment syndrome signs and your physician labels it shin splints with no stress check, ask particularly about persistent exertional compartment syndrome and request a referral for exercise-based stress measurement.
The stress check is mildly uncomfortable however transient, and it closes the diagnostic query definitively.
Does Surgical procedure for Compartment Syndrome Really Work?
For runners who wish to proceed coaching at earlier ranges, fasciotomy has the strongest proof of any accessible remedy.
The process includes making small incisions to launch the fascial sheath of the affected compartment, creating everlasting room for the muscle to broaden throughout train.
Research report that anterior compartment fasciotomy permits 60 to 80 p.c of runners to return to their earlier stage of coaching, with decrease success charges for deep posterior compartment releases.
In roughly 10 p.c of circumstances, signs return inside months as a result of the preliminary fascial launch was inadequate.
A second process is often wanted when recurrence occurs.
Restoration timelines are quicker than most critical working accidents: incisions heal inside one to 2 weeks, pool working and biking can start instantly after, and most runners are again on roads at six to eight weeks post-surgery.
RunnersConnect Bonus
Obtain our Prime 5 workouts to forestall anterior tibialis.
It’s a PDF with photographs and descriptions of the 5 simplest prevention and rehab workouts for runners with anterior tib points.
Can You Deal with Compartment Syndrome With out Surgical procedure?
Relaxation, anti-inflammatories, and foam rolling present momentary reduction however don’t resolve the stress drawback as soon as you come back to full coaching quantity.
One promising non-surgical different is a gait change.
A 2012 research from researchers at West Level examined whether or not transitioning to a forefoot strike may scale back anterior compartment stress sufficient to eradicate signs.
Researchers discovered that ten runners with anterior compartment syndrome who transitioned to forefoot putting over six weeks decreased post-run compartment stress by greater than half, with ache enhancements maintained at a one-year follow-up.
The mechanism is mechanical: heel-strike adopted by foot slap locations peak load on the anterior shin muscle tissues at each footfall.
A forefoot or midfoot strike distributes that load in a different way, lowering peak stress within the anterior compartment throughout the loading section.
Three caveats matter earlier than you do that:
- Proof is restricted. This was a single research with ten members and no management group. The outcomes are promising however not but definitive.
- Compartment specificity. This strategy solely applies to anterior compartment syndrome. For posterior compartment syndrome, forefoot putting will increase loading there and would worsen signs.
- Transition harm danger. Speeding a foot-strike change raises the danger of calf pressure, Achilles tendinopathy, and metatarsal stress fracture. A six- to eight-week transition with skilled steering is important.
If you wish to do that route earlier than surgical procedure, work with a physio or working coach to information the transition, then retest compartment stress after six weeks of constant forefoot working to see whether or not the intervention has decreased stress to regular ranges.
How Do You Prepare and Return to Working After Compartment Syndrome?
Aqua jogging is the best cross-training software throughout compartment syndrome restoration as a result of it replicates working mechanics in a zero-impact atmosphere.
Analysis exhibits that runners who practice completely with deep water working for 4 to 6 weeks keep cardio health and lactate threshold with no measurable decline in race efficiency once they return to land.
Stationary biking works as a secondary possibility if pool entry is restricted, although it develops totally different muscle activation patterns and doesn’t keep working economic system as successfully.
Begin aqua jogging instantly, whether or not you’re ready for a surgical date, recovering post-surgery, or trialing the forefoot strike strategy. There isn’t any profit to finish relaxation when a fitness-preserving different is out there.
Return-to-running timelines rely upon the remedy route:
- Submit-fasciotomy: Pool working or biking as soon as incisions heal (week one to 2); gradual return to street working beginning at week six to eight; full coaching load by weeks ten to 12
- Forefoot strike transition: Variable. Consequence will depend on how stress normalizes and the way your legs adapt; retesting compartment stress after six weeks of constant forefoot working offers you a concrete reply on whether or not to proceed or pursue surgical procedure
Three months from surgical procedure to full mileage is a sensible and customary consequence for anterior compartment syndrome, which is a quicker timeline than restoration from a tibial stress fracture or a big tendon harm.